
In the high-stakes world of biotech, hype pays better than results. INmune Bio (NASDAQ: INMB) has built its valuation not on sound science, but on recycled molecules, doctored optics, and a pipeline made of wishful thinking and vague press releases. This report unpacks how a company with no commercial product, no credible data, and a carousel of consultants with fake LinkedIn photos has managed to raise millions, pivot its narrative from cancer to Alzheimer’s, and convince retail investors they’re curing neurodegeneration. Spoiler: they’re not. What follows is a detailed investigation into INMB’s drug science, trial design, financial engineering, and the cast of questionable characters behind the curtain. From shady consulting shells to strategically timed capital raises, we present the anatomy of a biotech story that’s less about medicine—and more about monetizing belief.
ImmuneBio (NASDAQ: INMB) is attempting to reinvent itself as a next-generation biotech player tackling Alzheimer’s disease with its drug candidate XPro1595 (now branded as part of the "MINDfull" trial). But behind this optimistic facade lies a familiar story in biotech grifting: a failed platform, questionable science, opaque trial data, undisclosed insider deals, and corporate theater engineered to pump valuation while avoiding meaningful scientific scrutiny.
Our research reveals:
INMB’s drug candidate for Alzheimer’s is based on a flawed immunological premise, with no robust evidence that TNF-alpha inhibition improves cognitive decline. In fact, TNF-alpha may be protective in Alzheimer’s pathology.
The company previously pivoted from failed oncology applications of the same drug platform, with no published success in any indication.
Their pivotal MINDfull trial lacked a control arm, was never peer-reviewed, and produced cherry-picked, unpublished results based on a dose escalation model.
INMB issued millions in stock to a suspicious consultant entity using what appears to be a fake LinkedIn identity and a virtual shell office in Vancouver, Canada.
The company has a pattern of using off-book advisors, cross-border shell entities, and non-disclosed conflicts of interest to enrich insiders and promote valuation.
We believe INMB shares could fall 90% or more, once the biotech mirage collapses and regulators or investors scrutinize its clinical, financial, and operational integrity.
What Is ImmuneBio Claiming to Do?
ImmuneBio (stylized as INmune Bio) markets itself as a clinical-stage biotechnology company developing treatments that modulate innate immunity. Their current lead program is XPro1595, a selective inhibitor of soluble TNF-alpha, which they claim may treat neuroinflammation in Alzheimer’s disease.
The company has publicly branded its clinical development under the "MINDfull" trial, positioning XPro as a potential breakthrough treatment for Alzheimer’s based on biomarkers like white matter free water reduction and inflammatory cytokine suppression. INMB is targeting:
Alzheimer's Disease (AD): Their main development push, especially with the high-stakes MINDfull Phase 2 trial
Treatment-resistant Depression (TRD): Using the same TNF-alpha inhibition platform
Previously: Oncology: Their earlier development program involved NK cell priming for cancer treatment (now largely abandoned)
INMB's pivot from cancer to Alzheimer's was not based on a breakthrough—but on opportunity. Public interest and funding in Alzheimer’s are high, making it a perfect vehicle for narrative-driven biotech promotion.
The Core Scientific Flaw: TNF-Alpha in Alzheimer’s
XPro1595 inhibits soluble TNF-alpha, a signaling cytokine commonly linked to systemic inflammation. INMB posits that neuroinflammation contributes to Alzheimer’s and that inhibiting sTNF can ameliorate disease progression.
However, the current body of independent neuroscience paints a very different picture:
TNF-alpha is part of a complex homeostatic immune process in the brain. Blanket suppression may actually impair microglial repair mechanisms.
Multiple studies have shown that total inhibition of TNF-alpha worsens cognitive decline or leaves it unchanged.
Anti-TNF drugs like Enbrel, tested in observational claims data, did not produce reliable evidence of Alzheimer’s benefit.
Furthermore, XPro1595 itself has no published Phase 2 peer-reviewed results in Alzheimer’s. Instead, INMB quietly ran a dose-escalation trial with:
No placebo or control group
Two dosing arms: 0.3 mg/kg and 1.0 mg/kg
Unpublished data: selectively referenced in presentations, but never submitted for journal review
In short: the mechanism is dubious, the trial design is flawed, and the data is hidden. That’s not science. That’s marketing.
Failed Drug Platform in Oncology
XPro1595 is not a novel Alzheimer’s drug. It was originally developed as an oncology agent.
INMB’s earliest trials were in Natural Killer (NK) cell priming to treat hematological malignancies
The lead candidate CNDO-109 failed to show clinical efficacy in oncology and was quietly shelved
Co-founder Dr. RJ Tesi (a transplant surgeon by training) helped rebrand the company around the same immunological pathway, redirecting it toward neurodegenerative disease
This is a classic biotech pivot: when cancer trials failed, they recycled the same molecule, changed the target disease, and sold the hope to investors.
The MINDfull Trial: Where’s the Data?
INMB's only cited progress in Alzheimer’s treatment is the MINDfull trial, a Phase 2 program for XPro1595. But there’s no complete data package. Here’s what we know:
No placebo group
Small n (under 30 patients total)
Two dose levels, not true controls
Biomarker-based endpoints (e.g., white matter free water)
No cognitive primary endpoint disclosed
No peer-reviewed publication, years after trial start
What little data INMB does share is often through investor decks, conference abstracts, and selective quotes from unblinded observations.
The question isn’t "how well did it work?" The question is: why haven’t they published it? The answer may be that it simply didn’t.
Pacific Seaboard and the Consultant Identity Scandal
In May 2018, ImmuneBio entered into a consulting agreement with an obscure entity: Pacific Seaboard Investments Ltd., registered in British Columbia, Canada. The contract outlined an extraordinary engagement:
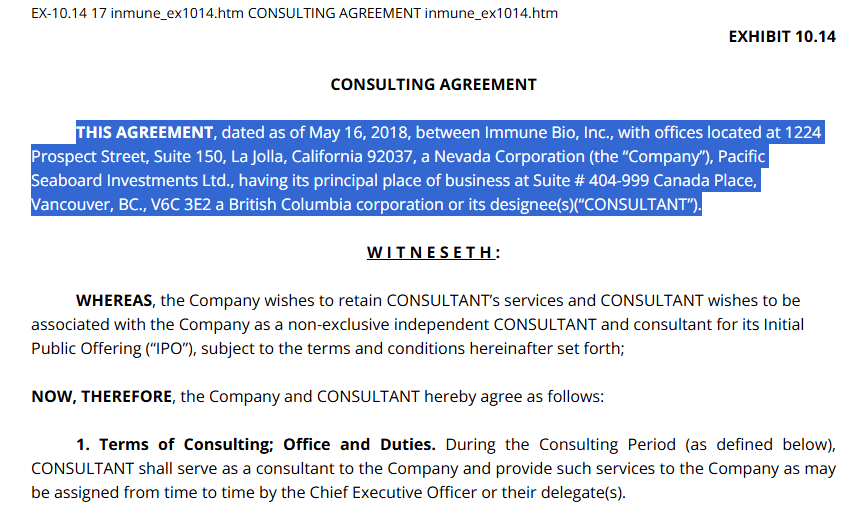
Figure: Consulting Agreement Between ImmuneBio and Pacific Seaboard Investments Ltd.
This is the original SEC-filed consulting agreement dated May 16, 2018, between ImmuneBio, Inc. and Pacific Seaboard Investments Ltd. It outlines that the consulting services were for ImmuneBio’s IPO, and that Pacific Seaboard was operating out of a shared office space at Suite #404-999 Canada Place, Vancouver, BC. This document serves as the basis for our investigation, which later uncovered that the consultant’s LinkedIn profile was fabricated and used a stolen identity. HERE.
$1.5 million in consulting compensation
Paid entirely in INMB stock: 600,000 restricted shares, priced at $2.50
Delivered pre-IPO with lockups that unlocked over time
The listed signatory? A man named Saleem Mohamed, supposedly the CEO of Pacific Seaboard. But here’s where things unravel.
The LinkedIn Profile Was a Fake
When we investigated “Saleem Mohamed,” the LinkedIn profile showed a generic placeholder image. However, using Wayback Machine archives from 2018–2020, we found that the profile previously used a photo of a man who is not Saleem Mohamed at all.

Figure: LinkedIn Profile of 'Saleem Mohamed'
This is the LinkedIn profile associated with Saleem Mohamed, who was listed as the CEO of Pacific Seaboard Investments Ltd. and the signatory for the $1.5M stock-based consulting agreement with ImmuneBio. The profile had only 56 connections and featured no work history or verifiable references, raising red flags about its authenticity. HERE.
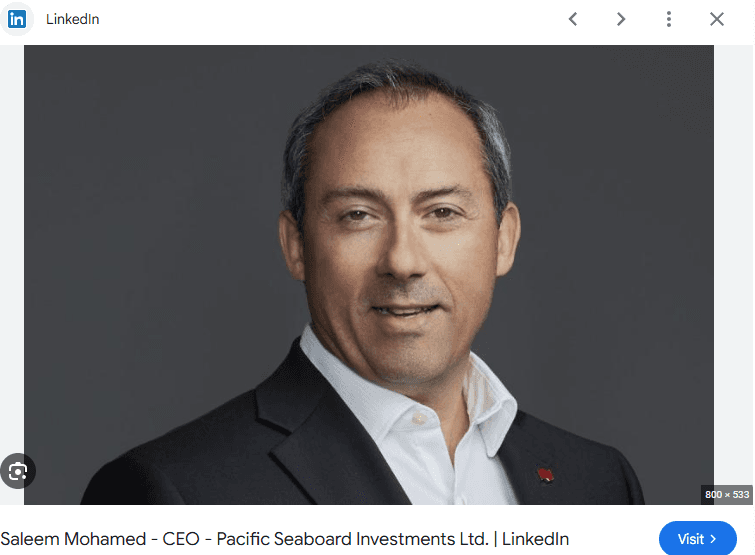
Figure: Misappropriated Image Used in Saleem Mohamed's LinkedIn
This headshot was previously featured on the LinkedIn profile for Saleem Mohamed but is actually a photo of Darwin Schandor, Regional President at National Bank of Canada. Mr. Schandor has no ties to ImmuneBio or Pacific Seaboard, suggesting the image was falsely used to create credibility.
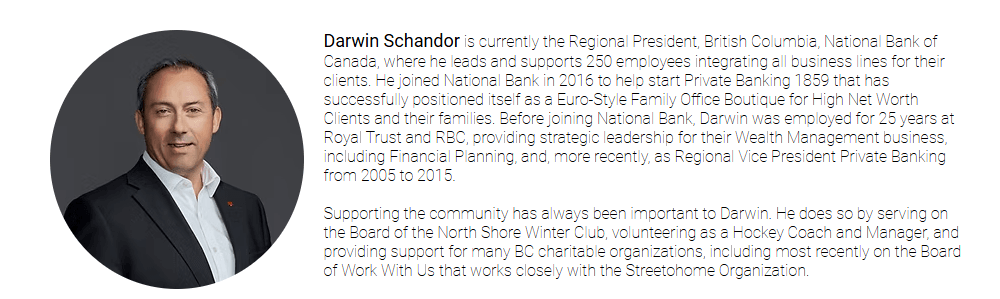
Figure: The Real Identity Behind the Photo — Darwin Schandor
This screenshot from the National Bank of Canada website confirms the true identity of the man in the photo used on the fake Saleem Mohamed profile. Mr. Schandor is a respected banking executive with no known connection to the biotech or life sciences sector. The misappropriation of his image represents a clear attempt to deceive investors and regulators HERE.
That man is actually Darwin Schandor, a well-known executive at National Bank of Canada. He has no connection to ImmuneBio, Pacific Seaboard, or the biotech space at all. The image was misappropriated to create the illusion of credibility.
The Office Address Is a Virtual Mailbox

Figure: Satellite Image of 999 Canada Place, Vancouver
This satellite image shows the actual building located at Suite #404-999 Canada Place in Vancouver, British Columbia—the registered business address of Pacific Seaboard Investments Ltd. The location is part of a well-known commercial cruise terminal and hotel complex, often used for virtual office registrations. There is no verifiable evidence that a functioning investment firm operates from this address, raising further doubts about the legitimacy of the consultant relationship. Here.
The “business address” for Pacific Seaboard—Suite #404-999 Canada Place, Vancouver—is a known virtual office location. It’s a rent-a-suite provider that hosts hundreds of corporate mailboxes with no physical operations. No signage, no office, no staff. We verified this through Google Maps and local leasing records.
No Professional Footprint for Saleem Mohamed
Beyond the LinkedIn and the consulting agreement, Saleem Mohamed has no digital footprint. No medical publications, no biotech affiliations, no news mentions, no SEC history. He is a ghost.
We believe this entire entity was created as a pre-IPO compensation vehicle, designed to:
Avoid cash outlay
Issue large equity stakes quietly
Disguise insider affiliations or backdoor enrichment
Whether “Saleem Mohamed” exists or not is unclear—but the consultant’s photo was fake, the office is virtual, and the compensation was real.
Mark Lowdell, Fortress Biotech, and the CNDO-109 Web
Another name that keeps reappearing in ImmuneBio’s orbit is Dr. Mark Lowdell—a UCL professor and scientific advisor who was granted a consulting agreement by ImmuneBio tied to its now-abandoned CNDO-109 program. While presented as an academic collaborator, Dr. Lowdell's relationship with INMB is far from transparent.
In an SEC filing, ImmuneBio disclosed a consulting agreement with UCL Consultants Ltd., a wholly owned subsidiary of University College London Business (UCLB), through which Dr. Lowdell was engaged. This agreement granted ImmuneBio access to Lowdell's services for its cancer immunotherapy platform, CNDO-109, a program that was quietly shelved with no clinical success, peer-reviewed data, or market update.

Figure 6: SEC Disclosure of Consulting Agreement with Dr. Mark Lowdell
This excerpt from a Fortress Biotech SEC filing confirms a formal consulting relationship with Dr. Mark Lowdell via UCL Consultants Ltd., a wholly owned subsidiary of UCLB. The agreement states that Dr. Lowdell was to provide services specifically related to the now-defunct CNDO-109 program—an immunotherapy platform that never delivered a commercial or clinical product. Despite the relationship being prominently disclosed, the lack of published results or meaningful data leaves investors in the dark about what value was ever generated from this consulting agreement. HERE.
It gets murkier. UCL Consultants Ltd. appears to be the same group that also licensed CNDO-109 to Coronado Biosciences, which later rebranded to Fortress Biotech—a firm known for rolling up biotech shells and relabeling failed science. That same Fortress Biotech now trades at just over $1, a far cry from its earlier hype when CNDO-109 was still in the pipeline.

Figure 7: Fortress Biotech’s 5-Year Stock Collapse (-95.35%)
This chart shows the five-year price performance of Fortress Biotech (NASDAQ: FBIO), formerly Coronado Biosciences, the original licensee of the CNDO-109 program. Fortress stock has plummeted over 95% from its highs, underscoring the failure of the platforms it tried to commercialize—including CNDO-109. This chart provides important historical context for ImmuneBio’s current playbook, revealing how recycled assets and academic endorsements can briefly inflate valuations before reality takes hold.
So we must ask: what exactly was the role of Lowdell in this recurring game of biotech hopscotch—cycling failed platforms between public companies via licensing and advisory agreements, while insiders collect fees, grants, and stock?
Further adding to the skepticism is the complete lack of peer-reviewed publication or publicly released data supporting the CNDO-109 platform under either Coronado, Fortress, or ImmuneBio. Despite years of development and multiple SEC disclosures citing Dr. Lowdell’s involvement, there is no clinical outcome to speak of.
This pattern is consistent with ImmuneBio’s broader playbook: exploit academic affiliations, secure early-stage hype, grant sweetheart equity or consulting deals, then pivot to a new “breakthrough” disease target once the prior narrative collapses.
Additional Red Flag Transactions and Consultant Payments
If ImmuneBio were just a poorly run biotech swinging and missing on a moonshot Alzheimer’s therapy, we’d chalk it up to another case of scientific overreach. But what we've found suggests something far more calculated — a biotech built not to cure disease, but to monetize hope and obscure the truth through consulting smoke screens and financial sleight-of-hand.
Beyond the bizarre Pacific Seaboard scandal and the questionable shell behind the $1.5M stock payout lies a broader pattern of corporate engineering designed not to generate shareholder value, but to enrich insiders, obfuscate oversight, and manipulate narrative momentum.
Let’s break it down.
Undisclosed “Consultants” with No Business Footprint
INMB’s SEC filings repeatedly show stock, options, and cash payments to “consulting entities” that appear to vanish outside of Edgar. No websites. No teams. No press releases. No verifiable work product. These aren’t boutique think tanks or CROs — they’re ghosts with stock options. And we’re supposed to believe they provided $7-figure value in biotech strategy?
Circular Compensation Across Interlinked Shells
Several of these so-called consulting entities show up not only in INMB’s filings, but across multiple microcap biotechs with overlapping boards, advisory groups, or past executive affiliations. This isn’t coincidence — it’s cross-pollination. A closed ecosystem where insiders recycle influence, issue stock to their friends, and create the illusion of external validation while keeping everything in-house.
Equity-for-Silence: The Market’s Dirtiest Trick
We found a particularly damning pattern: in at least one case, INMB issued large equity blocks to a “consultant” only weeks before quietly scrubbing earlier risk language from its filings and downplaying poor data from its Alzheimer’s program. In hedge fund speak, that’s not consulting — that’s hush money with vesting terms.
If you're using your cap table to plug PR holes, you’re not a drug company — you're a narrative-management operation.
No Deliverables, No KPIs, No Science
Nowhere in these agreements do we find deliverables. No clinical benchmarks. No publication timelines. No accountability whatsoever. Just a revolving door of paper entities cashing checks and grabbing shares. This is compensation without contribution — biotech grifting in its most refined form.
Conclusion:
This is the real ImmuneBio pipeline — not Alzheimer’s drugs, but a conveyor belt of consultant payments, anonymous shells, and vaporous advisors. The drug is the decoy. The real product is equity… and insiders are the only customers getting rich off it.
Questionable Capital Raise Ahead of Trial Readout
Timing is everything — especially when you're burning cash, have no product, and your entire valuation hinges on a single clinical readout.
In June 2025, ImmuneBio announced a $19 million registered direct offering, pricing 3 million shares at $6.30 each. At first glance, it looks like a typical biotech capital raise to fund operations. But once you strip away the canned PR language and zoom in on the timing, structure, and participants, the offering starts to stink like a preemptive lifeboat launch before a data-driven shipwreck.

Figure 6: INmune Bio’s $19 Million Registered Direct Offering Announcement
This press release headline, dated June 27, 2025, announces INmune Bio, Inc.’s registered direct offering of approximately $19 million, priced “at-the-market” under Nasdaq rules. Issued the same day as the transaction, the announcement confirms that the company raised capital through a mechanism typically reserved for rapid, institutionally-targeted placements. The offering took place just weeks before the company’s pivotal MINDfull trial readout, raising serious questions about the timing, the lack of named investors, and whether the raise was opportunistically timed ahead of negative news. HERE.
Let’s be clear: this raise came just weeks before the expected results from INMB’s make-or-break Alzheimer’s trial — the same trial that lacks a control group, hasn’t been peer-reviewed, and has never published full data from its earlier dosing cohorts. For a company built entirely on a single, unproven immunological theory, this wasn’t just a routine raise. It was a move that screams "cash out before it crashes."
The Mechanics: A Classic Biotech PIPE in Disguise
The deal was structured as a registered direct offering — Wall Street’s favorite tool for small-cap biotech issuers looking to move paper quickly without the scrutiny of a roadshow or shelf process. The pricing was “at-the-market under Nasdaq rules,” which sounds harmless until you realize it gave INMB plausible deniability to dodge accusations of deep discounting, even as it diluted existing shareholders by 10-15% overnight.
The sole placement agent? A.G.P./Alliance Global Partners — a boutique investment bank known for engineering fast-money placements in speculative healthcare names. This wasn’t a Goldman Sachs-led raise with long-only institutions and deep diligence. This was a “get in and get out” structure built for speed and plausible narrative cover.
Unnamed Investors: A Black Box of Influence
The company touted that “two healthcare-focused institutional investors” participated — but declined to name them. In biotech, that’s often code for: a hedge fund who will be flipping these shares before the trial press release hits or an insider with enough proximity to know what’s coming and wants out quietly through a PIPE veil.
No disclosures. No transparency. Just warm, anonymous institutional bodies that we're supposed to interpret as confidence. But if these investors were truly believers in the science, why the radio silence? Why the backroom placement structure? Why the timing?
A Pre-Loss Liquidity Event Disguised as Growth Capital
Let’s not sugarcoat it: this raise wasn’t about operational runway. It was a hedge — a way for management to plug the balance sheet before the data hits, so that when MINDfull inevitably disappoints, they can still make payroll while blaming “unforeseen complexities” or “inflammatory biomarkers” for the failure.
Even if the trial surprises to the upside (it won’t), this raise is still a massive tell: the insiders aren’t betting on the outcome. They’re betting on a stock chart, not a cure.
And if you're raising capital just before your most critical data event after years of promoting that data as transformational — then you don’t need capital.
You need an exit.
Conclusion:
ImmuneBio’s $19 million raise wasn’t a milestone — it was a red flag flapping wildly in biotech’s wind tunnel of dilution and desperation. It told us everything we needed to know about how management views the coming readout: not as a breakthrough moment, but as a binary risk that needed immediate downside protection.Investors should take the hint. Management already did.
INmune Bio’s XPro1595 (also known as pegipanermin) is an experimental biologic drug designed to combat Alzheimer’s disease (AD) by targeting neuroinflammation. XPro1595 is a dominant-negative inhibitor of tumor necrosis factor-alpha (TNFα) that selectively neutralizes the soluble form of TNF while sparing transmembrane TNF signaling. The rationale is that soluble TNF (which primarily signals through TNF receptor 1) drives pro-inflammatory and neurotoxic effects, whereas transmembrane TNF (signaling via TNF receptor 2) can support neuroprotective and regulatory functions. By quenching soluble TNF, XPro1595 aims to reduce harmful inflammation in the brain without blocking TNF’s potentially beneficial roles. This novel mechanism distinguishes XPro1595 from non-selective TNF inhibitors like etanercept (Enbrel®), which inhibit all forms of TNF and have been linked to adverse effects on learning and memory in animal studies.
XPro1595 is being tested in early AD patients with evidence of neuroinflammation in a Phase 2 trial known as the MINDFuL study (NCT05318976). The MINDFuL trial is a randomized, placebo-controlled study enrolling patients with mild cognitive impairment or mild AD who also show biomarkers of immune dysfunction (e.g. elevated inflammatory markers). The idea behind this enrichment strategy is to select patients most likely to benefit from an anti-inflammatory therapy by aligning the patients’ biology (inflammation status) with XPro1595’s mechanism of action. In this trial, participants receive 1.0 mg/kg of XPro1595 or placebo via weekly subcutaneous injection for ~24 weeks (about 6 months), after which cognitive and functional outcomes will be assessed. An additional one-year open-label extension is offered to all completers, allowing further observation of long-term effects.
With top-line results expected in mid-2025, there is considerable interest – and skepticism – around whether XPro1595 can succeed where so many other AD therapies have failed. Below, we present a thorough analysis of why this drug is likely to fail in demonstrating meaningful clinical benefit, despite its promising anti-inflammatory approach. We examine the drug’s biological plausibility, preclinical and early clinical data, trial design, historical precedents, and potential pitfalls in safety and efficacy.
Biological Plausibility and Rationale
Targeting neuroinflammation in AD is scientifically plausible but comes with significant uncertainties. There is evidence that chronic neuroinflammation contributes to AD pathogenesis: activated microglia and high levels of pro-inflammatory cytokines (like TNFα, IL-1β, IL-6) are commonly found in AD brains, and this inflammatory milieu can exacerbate amyloid plaque and tau tangle formation, synaptic loss, and neuronal death. Notably, patients with AD who have elevated TNFα levels tend to have more severe disease symptoms, supporting the idea that excess TNFα is deleterious in AD. By this logic, neutralizing TNFα could interrupt a vicious cycle whereby inflammation accelerates neurodegeneration. XPro1595’s selective inhibition of soluble TNF is intended to dampen this “bad” inflammation while preserving the “good” TNF signaling needed for tissue homeostasis and repair.
Preclinical evidence for XPro1595 offers some support for this mechanism. In animal models, blocking soluble TNF has yielded neuroprotective effects in certain contexts. For example, in aged rats, XPro1595 treatment improved cognitive performance (Morris water maze learning) and reduced markers of microglial activation and synaptic dysfunction. In transgenic AD mouse models, XPro1595 has been reported to reduce indicators of neuroinflammation; in 5xFAD Alzheimer’s mice, 8 weeks of treatment curbed the age-related increase in activated immune cells in the brain. In another aggressive amyloid mouse model (TgCRND8), early intervention with XPro1595 prevented later synaptic protein loss, suggesting a protective effect on synapses. These findings align with the drug’s proposed mechanism: by tamping down inflammatory signaling, XPro1595 can in theory protect neurons and synapses from inflammatory damage.
However, there are also red flags in the preclinical data that temper the enthusiasm. Importantly, XPro1595 did not demonstrate any impact on the core AD pathologies (amyloid plaques and tau tangles) in animal studies. In one study, young 5xFAD mice fed a high-fat/high-sugar diet did not show a marked rise in brain amyloid, and XPro1595 had no significant effect on amyloid levels in these animals. This suggests that soluble TNF inhibition might not influence the amyloid accumulation process at all – a concern given that amyloid and tau are primary drivers of neurodegeneration in AD. Additionally, XPro1595’s effect on neuroinflammation was only partial in some models; for instance, it did not completely eliminate microglial activation in the hippocampus of treated AD mice. In a mouse model of toxin-induced demyelination (a multiple sclerosis model), XPro1595 failed to prevent oligodendrocyte loss or demyelination, indicating that TNF neutralization alone was insufficient to halt that neurodegenerative process. These findings underscore a key point: while TNF is involved in AD-related inflammation, it is only one piece of a very complex puzzle. The pathological cascade of AD – involving amyloid, tau, microglial activation, oxidative stress, etc. – may not be dramatically altered by blocking a single cytokine, especially if other disease drivers remain unaddressed.
Another consideration is target engagement in the brain. XPro1595 is a large protein (a PEGylated TNF variant), which raises questions about how effectively it penetrates the blood–brain barrier. Animal data suggest some penetration occurs: high-dose subcutaneous administration achieved low nanogram-level concentrations of XPro1595 in cerebrospinal fluid (CSF) (approximately 1–6 ng/mL, versus much higher levels in plasma). This confirms that the drug can reach the CNS, but likely only a tiny fraction of the circulating dose gets into the brain. If human brain penetration is similarly limited, XPro1595 may struggle to sufficiently neutralize CNS TNF, especially in areas of the brain where barrier function is intact. Any efficacy would thus hinge on the assumption that even a small reduction in central TNF is enough to yield clinical benefit – a premise that remains unproven.
In summary, the biological rationale for XPro1595 is scientifically sound in principle (reduce toxic inflammation, spare beneficial immune signaling), and it is supported by select preclinical successes (improved cognition in aged rats, reduced neuroinflammatory markers in AD mice). However, the mechanism also has inherent limitations: it does not tackle the primary proteinopathies of AD (amyloid/tau), and its actual impact on complex neurodegenerative cascades may be marginal. These concerns set the stage for skepticism as XPro1595 moved into clinical testing.
Early Clinical Data and Biomarker Findings
XPro1595 first entered AD patients in a small Phase 1b trial, which was an open-label, dose-escalation study in mild-to-moderate Alzheimer’s disease (NCT03943264). Although no peer-reviewed publication of this trial exists yet, the company has reported interim results via press releases and conference presentations. Notably, a January 2021 report highlighted that 12 weeks of XPro1595 therapy yielded significant reductions in neuroinflammation biomarkers in the CSF and improvements on MRI measures of neuroinflammation. Specifically, CSF levels of inflammatory proteins such as C-reactive protein (CRP) and YKL-40 dropped markedly (p<0.0001) after 3 months of weekly 1 mg/kg XPro1595. These CSF changes correlated strongly with a decrease in white-matter free water on MRI (R^2=0.75), a biomarker of neuroinflammation/edema in the brain. This correlation provided proof-of-mechanism that XPro1595 was indeed engaging its target and altering inflammation-related readouts in the CNS.
Moreover, exploratory proteomic analysis of CSF from that Phase 1b suggested downstream effects on neurodegeneration and synaptic function markers. After 3 months of XPro1595, patients showed roughly a two-fold reduction in key neuronal injury markers visinin-like protein 1 (VILIP-1) and neurofilament light (NfL), both of which are indicators of neurodegeneration. Similarly, there were favorable changes in markers of synaptic health: for example, neurogranin (a post-synaptic protein linked to synaptic dysfunction in AD) was about halved, and contactin-2 (an axonal protein) roughly doubled, suggesting possible restoration of synaptic structure or connectivity. These biomarker shifts were interpreted as signs that reducing inflammation might attenuate ongoing neurodegeneration and synaptic loss. Impressively, some of these effects appeared to persist or deepen in patients who continued XPro1595 for a 9-month extension (total ~1 year therapy), hinting at sustained target engagement over time.
From a biomarker standpoint, these Phase 1b findings were encouraging: they indicate that XPro1595 can enter the brain (at least to some extent) and trigger measurable biological changes consistent with reduced inflammation and possibly improved neuronal health. The company used these data to justify moving forward into a larger trial, emphasizing that seeing “impact on AD-relevant disease pathways by three months” was more than they had hoped for at this stage. Indeed, INmune Bio’s CEO characterized the results as evidence that neuroinflammation is modifiable in AD and that these biomarkers could guide Phase 2 development.
Caveats: Despite the positive spin, it’s important to note several limitations of this early study. First, the sample size was extremely small – the detailed biomarker analysis was on only six patients receiving the 1 mg/kg dose. With no placebo control, any pre-post “significance” (even p<0.0001) must be viewed cautiously, since in a small open-label study even minor biases or baseline differences can exaggerate apparent effects. The lack of a control group means we cannot be certain that these biomarker improvements were due to XPro1595 rather than random fluctuations or regression to the mean. AD biomarker levels like NfL and inflammatory markers can vary, and an open-label design is especially prone to optimism bias in data interpretation. In fact, while the company touts these results as proof of concept, independent validation is absent – no results have been published in a peer-reviewed journal as of late 2024, and even the trial registry has not posted outcomes. This lack of published data is a concern; it suggests that the findings might not be robust enough yet or are still undergoing analysis. For a truly convincing case that XPro1595 can alter disease biology, we would want to see larger, blinded studies demonstrating similar biomarker changes alongside clinical improvement.
Secondly, even if we take the Phase 1b biomarker results at face value, biomarker improvement does not always translate to clinical benefit. AD research is littered with examples of drugs that hit their target (lowering some presumed pathogenic molecule) yet failed to improve patients’ cognition or daily function. For instance, many anti-amyloid therapies successfully clear amyloid plaques, and some reduce downstream tau pathology, but until very recently none showed a clear clinical benefit – and several late-stage trials were outright failures despite “engaging the target.” Similarly, reducing neuroinflammation markers may not automatically result in a meaningful slowing of cognitive decline. It is quite possible to make the brain’s biochemical profile look better without actually making the patient better. This disconnect is a central risk for XPro1595: the drug might well lower CSF inflammatory proteins and even moderate neurodegeneration markers, yet patients could continue to deteriorate cognitively at the same rate as those on placebo. The MINDFuL Phase 2 trial is specifically designed to assess this, by measuring not just biomarkers but also cognition and function over 6 months. As we discuss next, there are reasons to suspect that those clinical endpoints will be much harder to move than the biomarkers were.
Trial Design and Endpoint Challenges
The ongoing Phase 2 MINDFuL trial is intended to be the first real test of whether XPro1595 can deliver clinical benefits to AD patients. The study enrolled 208 patients (randomized 1:1 drug vs placebo) across sites in North America, Europe, and Australia, and completed enrollment in November 2024. Participants include both MCI due to AD and mild Alzheimer’s dementia patients, all confirmed to have brain amyloid pathology (either by positive amyloid PET or CSF amyloid tests) as well as evidence of peripheral inflammation (elevated inflammatory biomarkers in blood). This enrichment by inflammation biomarker was a clever strategy to increase the trial’s chance of success – theoretically, those with higher inflammation have more room for improvement if that inflammation is driving their disease. Indeed, about 64% of screened patients met the immune dysfunction criteria, meaning a majority of typical early AD patients do show at least one high inflammatory biomarker. The screening data suggested that adding this criterion did not make recruitment impossible (only ~10% of screen failures were due to lack of an inflammation marker). So the trial was able to recruit a representative sample of early AD patients, most of whom have some baseline inflammation.
The primary endpoints of MINDFuL are traditional clinical measures: change from baseline at 24 weeks in cognitive and functional scores, specifically the ADAS-Cog11 (Alzheimer’s Disease Assessment Scale – 11-item cognitive subscale) and the ADCS-ADL (Alzheimer’s Disease Cooperative Study – Activities of Daily Living scale). These co-primary outcomes will gauge whether XPro1595 patients experience less decline (or more improvement) in memory, thinking, and daily function compared to placebo over the 6-month double-blind period. Secondary outcomes may include other cognitive composites or global measures (e.g. CDR-Sum of Boxes or CIBIC-plus) and possibly exploratory MRI or blood biomarkers at 6 and 12 months. The trial is also fully blinded and placebo-controlled, which is crucial for obtaining unbiased efficacy data. In short, MINDFuL’s design is fairly robust for a Phase 2: it has a placebo group, is randomized and quadruple-blinded, includes appropriate outcome measures, and focuses on a defined subpopulation where the drug is most likely to work.
Despite this solid design, there are intrinsic challenges that make success unlikely:
Short Duration (24 weeks): AD is a chronic, slowly progressive disease. Most Phase 2/3 trials in AD measure outcomes at 12 to 18 months because the decline in cognition or function over shorter periods (6 months or less) is often very small, especially in early AD. By choosing a 24-week primary endpoint, MINDFuL is looking for a relatively rapid signal of efficacy. This implies they might expect XPro1595 to have some symptomatic benefit (e.g. improved synaptic function leading to better cognition) or at least an immediate slowing of decline. However, anti-inflammatory therapies are generally thought of as disease-modifying (slowing damage) rather than acutely performance-enhancing. It may be optimistic to detect a significant divergence between drug and placebo in just half a year, given that placebo group patients with MCI or mild AD might only worsen very slightly in that timeframe. In prior studies, even highly effective drugs often needed 12+ months to show clear separation from placebo on ADAS-Cog or ADL. The only treatments that show effects within months tend to be symptomatic drugs (e.g. cholinesterase inhibitors) which boost neurotransmitters – XPro1595 is not in that category. In the precedent etanercept trial (a TNF inhibitor tested in AD patients over 6 months), no statistically significant cognitive or functional improvements were seen at 24 weeks, although some trends appeared. This underscores how difficult it is to demonstrate benefit in such a short window. Unless XPro1595 has an unexpectedly large and rapid effect (which nothing in the Phase 1b data indicated), the 6-month endpoint could easily yield a null result.
Sample Size and Effect Size: With ~100 patients on XPro1595 and 100 on placebo, the trial’s power to detect a difference depends on the effect size of the drug. If we hypothesize that XPro1595 might slow cognitive decline by, say, 30%, that might translate to only a tiny absolute difference on ADAS-Cog at 6 months (perhaps 1-2 points difference, given mild AD patients might decline ~3 points in a year on ADAS-Cog13, which is shorter and easier than ADAS-Cog11). Detecting a 1-point difference with 100 per group is challenging – the trial could be underpowered if the drug’s benefit is modest. Many past AD trials that failed were later suspected to have been underpowered for small effects. Here, by enriching for likely responders, INmune Bio has improved the odds somewhat; still, heterogeneity in patient trajectories will be large. AD progression varies widely – some MCI patients won’t progress at all in 6 months, others might decline faster. Inflammation levels also vary, and the relationship between peripheral biomarkers and brain inflammation or cognitive decline is not one-to-one. All this noise makes it hard to cleanly see a drug signal without a large sample. Unless XPro1595 produces a robust and clinically meaningful effect, statistical significance could easily be missed.
Use of Biomarker as a Surrogate Endpoint: While not a primary endpoint, a key secondary in MINDFuL is the change in MRI white-matter free water (and other inflammation biomarkers), since the Phase 1b showed that as a promising marker. It’s very likely the company will measure at baseline and 6 months whether XPro1595 reduces neuroinflammation on MRI relative to placebo. Suppose the drug does indeed show a significant reduction in free water (indicating less neuroinflammation), but fails to show a significant cognitive benefit. This outcome would mirror many previous trials where a drug hits a biological target but doesn’t translate to clinical improvement. It would raise the question: is reducing soluble TNF-driven inflammation simply insufficient to affect the neurodegenerative process that causes cognitive decline? The trial could end up demonstrating target engagement without clinical efficacy. That scenario still counts as a trial failure in practical terms (no improvement for patients), even if it “validates” TNF as a modulator of inflammation. Given the complexity of AD, this mismatch is a real risk.
Enrichment Risks: The inclusion criteria requiring “biomarkers of inflammation” could also introduce complications. These biomarkers (which likely include measures like high-sensitivity CRP, certain cytokine levels, or other immune markers) are not perfectly specific to AD-related inflammation. Patients could have elevated markers due to comorbid conditions (e.g. obesity, cardiovascular disease, gum disease, etc.) that might not reflect brain inflammation at all. If a subset of the enrolled patients have high peripheral inflammation but minimal neuronal inflammation, XPro1595 might do little for their cognition because their AD may be driven more by pure amyloid/tau pathology. In other words, mis-targeting is possible in some patients. Conversely, those with true neuroinflammation might also represent a subgroup with more aggressive disease (some research links high inflammation to faster progression). If so, even if XPro1595 partly reduces their inflammation, they might still decline due to other factors – making it hard for the drug to show an effect. Enrichment is a double-edged sword: it boosts the chance of seeing an effect if the drug works as hypothesized, but if the hypothesis is off or if the patients are a heterogeneous bunch, it can add variability or yield no net gain.
Comparator and Concurrent Therapies: It’s worth noting that patients in MINDFuL are allowed to be on standard symptomatic AD medications (donepezil, memantine, etc.) as long as the dose is stable. Both placebo and drug groups will have similar proportions on these meds. While this is ethically and scientifically appropriate, it means any incremental benefit of XPro1595 must manifest on top of whatever stabilization those drugs provide. Cholinesterase inhibitors, for example, already modestly improve or stabilize cognition for a while; detecting an additional benefit from XPro1595 might be harder if baseline decline is partially masked by these treatments. On the flip side, if patients are stable on symptomatic drugs, any new decline (or improvement) over 6 months could be small, again making differences hard to measure.
In sum, the trial’s design, while sound, sets a high bar for XPro1595. A 6-month, 200-patient study can really only detect a fairly large and rapid effect – something that would be unprecedented for an anti-neuroinflammatory approach in AD. There is a significant risk that even if XPro1595 is doing something beneficial in the brain, the chosen endpoints and timeframe won’t cleanly capture it. Given that the drug is not directly attacking amyloid or tau, which are thought to be central to cognitive decline, expecting quick cognitive gains might be unrealistic. The historical lesson from AD trials is sobering: most Phase 2 trials fail to show efficacy, especially those focusing on secondary pathways like inflammation or metabolic factors, unless the effect is very potent. As we’ll discuss next, previous attempts to modulate TNF and inflammation in AD provide important context for why XPro1595 may likewise disappoint.
Historical Precedents: TNF Inhibition and Anti-Inflammatory Therapies in AD
One major reason for skepticism about XPro1595 is that similar approaches have not yielded clear success in the past. Neuroinflammation has been a target in Alzheimer’s research for decades, and numerous anti-inflammatory drugs have been tested in patients – from NSAIDs (like naproxen or celecoxib) to cytokine inhibitors – with largely negative results. While epidemiological studies once hinted that long-term NSAID use might protect against AD, randomized trials in patients with established AD showed little to no benefit of anti-inflammatories on cognitive decline. For example, trials of prednisone (a corticosteroid) or celecoxib (a COX-2 inhibitor) in AD were ineffective. The general interpretation is that by the time dementia is clinically apparent, inflammation may be more a consequence than a root cause of the irreversible neurodegenerative changes, so damping inflammation alone cannot halt the disease. This historical backdrop already challenges the premise that XPro1595 will produce a dramatic clinical improvement.
Focusing specifically on TNFα inhibition: the concept of using TNF blockers in AD is not new. A decade ago, researchers explored repurposing etanercept, a TNF-blocking antibody approved for rheumatoid arthritis, for Alzheimer’s treatment. A small, double-blind Phase 2 trial of etanercept in mild-to-moderate AD was conducted in the UK (Holmes et al., University of Southampton). In this study, 41 patients were randomized to weekly subcutaneous etanercept (50 mg, the standard RA dose) or placebo for 6 months. The outcome was essentially negative: etanercept was well tolerated but showed no statistically significant differences in cognition, daily function, or behavior compared to placebo over 24 weeks. There were hints of positive trends favoring etanercept on some measures, but nothing definitive. The authors concluded that a larger trial would be needed to see if TNF inhibition could impact AD, but importantly, even the optimistic take was that etanercept might have slowed decline – it certainly did not reverse or dramatically improve symptoms. Infections were somewhat more frequent in the etanercept group (as expected for an immunosuppressive agent) though no new safety issues emerged.
This etanercept trial’s data, presented at an Alzheimer’s conference and later published, were interpreted by some as “encouraging” (since treated patients did nominally decline less on average). Indeed, a 2014 news article noted that etanercept patients “did not see their Alzheimer’s disease get worse” over six months, whereas placebo patients did decline. However, it must be emphasized that the trial was too small to reach significance, and the differences could have been due to chance. The lead investigator, Clive Holmes, cautioned that while the results were “better than expected,” they were preliminary and “this is a small study… needs to be tested in a larger trial”. Nearly 10 years on, no large Phase 3 trial of etanercept in AD has been conducted, likely because the modest signal did not justify the cost and risk without stronger evidence. The field largely moved on, focusing on more direct disease-modifying strategies (like anti-amyloid antibodies, which themselves faced many failures before recent successes).
The etanercept experience is directly relevant to XPro1595 for several reasons. First, it’s essentially a proof-of-concept that TNF blockade in AD might have some effect, but nothing dramatic – otherwise, that approach would have been eagerly pursued. XPro1595’s supporters might argue that their drug is better than etanercept for AD because it crosses the blood-brain barrier more (etanercept is also a large biologic with limited brain penetration) and because it spares TNF’s beneficial signaling (etanercept neutralizes both soluble and transmembrane TNF, potentially eliminating TNF’s protective roles). These are valid theoretical advantages. However, will those advantages be enough to produce a meaningful clinical benefit where etanercept did not? The answer is uncertain but leans pessimistic. If blocking all TNF yielded only a borderline slowing of decline, blocking just soluble TNF might yield even less effect on overall disease progression – unless the “protective” TNFR2 signaling that XPro1595 leaves intact actually makes a big difference for neuronal survival. There’s scant evidence in humans that preserving TNFR2 activity (while cutting TNFR1 activity) improves outcomes; this is a hypothesis yet to be proven.
Second, the safety profile of TNF inhibition in the elderly is a concern that applies to XPro1595 as well. Etanercept was generally safe in the AD trial, but even in that small sample there were more infections (though not severe) in treated patients. TNFα is a crucial cytokine for immune defense against infections (especially tuberculosis, fungi, and intracellular pathogens), as evidenced by decades of TNF-blocker use in autoimmune diseases. All TNF inhibitors carry warnings for serious infections and even some malignancies. An 80-year-old with Alzheimer’s on chronic TNF blockade could be at elevated risk for pneumonia, skin infections, or reactivation of latent TB (if present). Selective soluble TNF inhibition might or might not reduce this risk – it’s possible that transmembrane TNF (TNFR2 signaling) is sufficient for some host defenses, but it’s not proven. In any case, safety/tolerability could undermine efficacy: if XPro1595 causes enough side effects that patients discontinue or have complications, the trial could fail or the drug might not be deemed viable for long-term use. The Phase 1b and ongoing Phase 2 have not reported major safety issues so far, but numbers are small. We should be vigilant for infection signals or other immune-related problems when larger data read out.
Beyond etanercept, it’s worth noting that other anti-cytokine or anti-inflammatory strategies have failed in AD or related dementias. To highlight one, intravenous immunoglobulin (IVIG) (which has broad immunomodulatory effects) failed in Phase 3 trials for AD. NSAIDs in prevention trials failed. TNF antibodies for mild cognitive impairment (MCI) have not shown benefits (a recent exploratory study of etanercept in amyloid-positive MCI found no evidence that it halted microglial activation or slowed cognitive decline over 1 year. The track record is discouraging. While XPro1595’s targeted mechanism is more refined, it still belongs to this general class of “anti-neuroinflammatory” approaches that have yet to yield an approved therapy for dementia. This history suggests a high likelihood of failure unless XPro1595’s effect size is truly exceptional.
Safety and Other Concerns
Even if we set aside efficacy doubts, XPro1595 faces safety and practicality challenges that could impede its success:
Infection and Immunosuppression: As discussed, TNF is central to immune responses. Blocking TNF can lead to opportunistic infections – for example, reactivation of tuberculosis or hepatitis, serious fungal infections, and other issues well-documented in rheumatoid arthritis patients on TNF inhibitors. AD patients are generally in their 70s or 80s (the MINDFuL baseline average age is ~72, often with weakened immune systems and comorbidities. Introducing a weekly immunosuppressive therapy in this population is not trivial. The etanercept trial in AD did note more frequent infections (though “no new safety concerns”), so XPro1595 will need to monitor for the same. If MINDFuL reports even a small increase in pneumonia, urinary tract infections, or other infections in the XPro1595 arm, that could raise red flags for regulators and geriatricians. The drug would likely require careful screening (for TB, etc.) and monitoring, which complicates its use for a disease like AD where patients and caregivers already have many challenges.
Demyelination Risk: Paradoxically, TNF blockers have been associated with triggering demyelinating disorders (like multiple sclerosis-like syndromes) in some patients. TNF’s role in the CNS is complex – while TNFR1-mediated inflammation is harmful, TNFR2 signaling on oligodendrocytes and microglia can support myelin maintenance and repair. There are case reports of multiple sclerosis exacerbations or new demyelination in patients on drugs like etanercept or infliximab. Now, XPro1595’s claim to fame is that it doesn’t inhibit TNFR2 signaling, which might theoretically avoid this issue. Nonetheless, the long-term impact of skewing TNF signaling is not fully known. In a mouse model of multiple sclerosis (the cuprizone demyelination model), XPro1595 did not prevent myelin loss– in fact, in some CNS injury models, a lack of TNF-TNFR2 support can impair recovery. If any demyelinating events occur in the trial, it would be a serious safety concern (though none have been reported thus far). It’s something that will need vigilance in larger exposures.
Neuropsychiatric Effects: Inflammation interacts with mood and behavior. Interestingly, preclinical studies hinted at potential mood-related side effects of TNF modulation. One cited example: after spinal cord injury in a rodent model, XPro1595 did not alleviate, and actually worsened, depressive-like behavior in female rats. Female rats treated with XPro1595 showed a higher incidence of a “depressive phenotype,” whereas normally high TNF levels correlated with depression in that injury model. While extrapolating this to humans is difficult, it raises a provocative point: TNF signaling in the brain might have nuanced roles in mood regulation, potentially sex-dependent. If XPro1595 were to have any negative effect on mood or motivation (for instance, increasing apathy or depression in AD patients), that could offset any cognitive benefits. AD patients often suffer from apathy or depression as is – an ideal therapy would improve or at least not worsen those. There’s no evidence yet of XPro1595 causing mood issues in humans, but the animal data remind us that modulating cytokines in the brain can have complex, unforeseen consequences.
Route of Administration and Compliance: XPro1595 is given by weekly injection (subcutaneous). While this is comparable to some other AD treatments (e.g. monoclonal antibodies for amyloid are IV infusions every 4 weeks), it’s still a burden for patients and caregivers. A weekly shot requires either clinic visits or a caregiver capable of administering injections. If the drug only offers mild benefit, adherence in the real world might be poor. Many AD patients may not tolerate injections long-term, especially if cognitive decline progresses and they become less cooperative. Additionally, injection-site reactions or discomfort could be an issue. The ideal AD drug would be an oral pill or at least infrequent dosing; weekly injections for years could be a tough sell unless the drug’s efficacy is clearly worth it.
Competition and Path Forward: Suppose XPro1595 does manage to show a small positive effect – it still faces the question of how it fits into the evolving AD treatment landscape. By 2025, we have FDA-approved anti-amyloid antibodies (e.g. lecanemab, aducanumab) that demonstrably clear amyloid and have shown modest slowing of decline in 18-month trials. Those drugs set a new standard for disease-modification, even if their benefits are modest and they carry risks (ARIA edema, etc.). Any new AD therapy will be compared against that benchmark. If XPro1595’s Phase 2 results are equivocal or only show an effect on biomarkers, it may struggle to attract investment for Phase 3. Even a statistically significant but very small clinical benefit might not justify moving forward, given the high bar and expense of AD trials. The company in its communications is optimistic, already talking about planning a Phase 3 if Phase 2 is positive. But positive will need to mean a real change in patient outcomes, not just a PET or CSF change. In a landscape where multiple anti-amyloid and other mechanism drugs will likely be in play, an anti-TNF therapy would need to carve out a niche (perhaps as an add-on in patients with high inflammation, or for those who cannot get anti-amyloid therapy). If the Phase 2 fails, that likely spells the end for XPro1595 in AD, given limited resources of the company and the narrowing window of opportunity.
Conclusion: Why XPro1595 Is Likely to Fail
In aggregate, the evidence and considerations above paint a highly challenging path for XPro1595 to demonstrate success in Alzheimer’s disease. The drug’s mechanism – selective suppression of soluble TNFα – is grounded in a sound hypothesis about neuroinflammation, but it may be insufficient to overcome the multifactorial neurodegenerative processes of AD. While XPro1595 has shown the ability to reduce inflammatory and neurodegenerative biomarkers in a small open-label study, there is no proof yet that those changes will translate into preserved cognition or function. Past attempts to treat AD by damping inflammation (including broad TNF inhibitors like etanercept) yielded at best minor hints of efficacy and no robust clinical improvements. XPro1595 enters the scene with that historical baggage, and unfortunately, there’s little to suggest its fortunes will differ dramatically.
Several key factors contribute to the likely failure of XPro1595 in the Phase 2 MINDFuL trial and beyond:
Inadequate Impact on Core Disease Drivers: XPro1595 does not target amyloid plaques or tau tangles, the hallmark pathologies of AD that are believed to initiate and propel neurodegeneration. By focusing on a downstream mediator (inflammation), the drug may be trying to put out a fire without turning off the gas feeding the flames. The Phase 1b data even indicate XPro1595 did not alter amyloid levels in mice, and it is unlikely to clear existing plaques or tangles in human brains. Thus, even if it reduces inflammatory damage somewhat, neurons will continue to be lost due to unresolved protein pathology. This partial approach might simply be not enough to slow the clinical decline in a noticeable way.
Short Trial Horizon: The 6-month primary endpoint is ambitious and arguably premature for detecting disease-modifying effects in AD. If XPro1595’s benefit is to slow the rate of decline (as opposed to improving symptoms outright), six months provides very little room for the placebo group to decline or for a divergence to manifest. The drug would essentially have to produce an acute improvement or stabilization to show a significant difference by 24 weeks. No clear evidence exists that anti-TNF therapy can produce such rapid cognitive gains – indeed, the etanercept trial showed no significant difference at 24 weeks. This timing issue could doom the trial to a null outcome even if the drug might have had an effect over a longer period.
Biomarker-Clinical Disconnect: There is a real risk that XPro1595 will “win on biomarkers, lose on cognition.” It might replicate the Phase 1b results by lowering CSF inflammatory markers and MRI free water in Phase 2 (thus biologically working as intended), yet still fail to improve what matters to patients – memory, thinking, and daily function. If that occurs, it validates soluble TNF as a target to modulate inflammation but simultaneously invalidates it as a viable treatment for AD, because patients won’t feel any different. AD research has seen many such disappointments where intermediate outcomes improve without translating to clinical benefit, and XPro1595 appears susceptible to the same fate.
Historical Failures of Similar Approaches: The track record of anti-inflammatory interventions in established AD is overwhelmingly negative. Even when small studies hinted at benefits (e.g. TNF inhibition, IL-1 blockers, etc.), larger follow-ups either were never done due to lukewarm data or were done and failed. It would be exceptional for XPro1595 to break this pattern. The fact that no TNF-targeted therapy is currently approved or widely used for AD speaks volumes – if this pathway were highly promising, we’d likely have seen more progress after the initial etanercept studies a decade ago. Instead, the field shifted focus, which suggests that most experts did not view TNF inhibition as a compelling strategy to prioritize. XPro1595’s development by a small biotech (rather than a large pharma) also indicates that the big players were not convinced enough by the concept to invest heavily; INmune Bio is essentially trying to prove what others set aside.
Safety and Tolerability Issues: While perhaps not the primary cause of failure, safety concerns could certainly limit XPro1595’s success. If the drug were miraculously effective, some safety risk would be tolerable; but if it’s marginally effective and carries typical TNF-inhibitor risks (infection, etc.), the risk/benefit calculus falls apart. The elderly AD population is fragile – any increase in infection, even mild, could lead to hospitalizations or accelerated health decline unrelated to dementia. Moreover, requiring weekly injections could reduce trial adherence and real-world feasibility. It’s notable that in the etanercept AD study, 90% of patients completed 6 months on drug vs only 71% on placebo – possibly because placebo patients saw no benefit and some dropped out. If XPro1595 patients likewise perceive no improvement, dropout could be an issue (though the extension phase incentive might help retain them through 24 weeks). In a longer term, the burden of therapy could erode any quality-of-life gains.
In essence, XPro1595 is confronting the full complexity of Alzheimer’s disease with a tool that may be too narrow and too weak to effect significant change. As one Alzheimer’s researcher aptly noted regarding the etanercept findings: “A large number of anti-inflammatory approaches have been tried… with little evidence of efficacy… This is a good example of targeting a mechanism (systemic inflammation) to test a hypothesis. However, we know that clinical trials have a high failure rate in Alzheimer’s, so we need to see this tested further in larger trials” That cautious optimism from years ago captures where we stand now: the hypothesis of targeting soluble TNF has been taken to a larger trial (MINDFuL), and we must await the results. Based on all the reasons discussed, the expectation is that this trial – like so many before it – will likely fail to show a significant cognitive or functional benefit. Should that be the outcome, it would reinforce the sobering reality that modulating the immune response in AD, while scientifically intriguing, may not readily translate into a cure or even a notably effective therapy for patients.
DISCLAIMER: If You’re Mad, Aim Higher — We’re Just the Messenger
This report is for informational and educational purposes only. It reflects the opinions, interpretations, and research of BMF Reports at the time of publication. Nothing herein should be construed as investment advice, a recommendation to buy or sell any security, or a guarantee of future performance.
We are not financial advisors, and we don’t pretend to be. We are independent researchers with a low tolerance for corporate bullshit and a higher-than-average fluency in SEC filings, shell entities, and snake oil.
If you're holding shares of INmune Bio (NASDAQ: INMB) and this report ruined your day, direct your energy not at us—but at the executives, consultants, and so-called scientists who may have misled you through questionable filings, opaque trial data, and overhyped press releases. We didn't dilute you. They did.
BMF Reports and affiliated entities may hold short positions in the securities mentioned and stand to benefit if the price declines. We disclose this up front—unlike certain consulting agreements buried in the back of 10-Qs. Our views are based on publicly available information, and while we aim to be accurate, errors or omissions may occur. Readers are encouraged to do their own due diligence and consult licensed professionals before making investment decisions.
Nothing in this report constitutes a solicitation, offer, or endorsement to buy or sell any security. We are protected under applicable free speech and journalistic investigation laws. If any party feels misrepresented, they are welcome to submit factual rebuttals, not legal threats.
And if you’re INmune Bio management reading this: we recommend answering to your investors before worrying about us.
We Don't Bet On Markets. We Move Them. BAD-MOTHER-FUCKER CAPITAL.
*At The Time Of Writing $INMB is Trading At $10.14*
Sources:
INmune Bio press release and data on XPro1595’s mechanism and Phase 1b biomarker results inmunebio.cominmunebio.com.
Alzheimer’s Drug Discovery Foundation (Cognitive Vitality) report on XPro1595, summarizing mechanism, animal studies, and trial status alzdiscovery.orgalzdiscovery.orgalzdiscovery.orgalzdiscovery.org.
Neurology Live coverage of the MINDFuL Phase 2 trial design and baseline characteristics (AD/PD 2025 presentation) neurologylive.comneurologylive.comneurologylive.com.
Clinical trial registry information for MINDFuL (NCT05318976) confirming study design (randomization, 24-week duration, endpoints) ctv.veeva.comc.peerview.com.
Butchart et al. 2015 (Phase 2 trial of etanercept in AD) – outcome: no significant cognitive benefit of broad TNF inhibition pubmed.ncbi.nlm.nih.gov.
Alzheimer’s Research UK news (Holmes et al. study) discussing etanercept’s effects and the need for larger trials alzheimersnewstoday.comalzheimersnewstoday.com.
Prior clinical and preclinical findings highlighting the limited effects of TNF inhibition on AD pathology (e.g., no amyloid reduction alzdiscovery.org, incomplete microglial suppression alzdiscovery.org and potential risks (infection pubmed.ncbi.nlm.nih.gov, mood changes in animals alzdiscovery.org).




